Broken Heart/Takotsubo Syndrome Complications
By Jeyashree Sundaram, MBA
Broken heart syndrome, or Takotsubo cardiomyopathy (TCM), is a temporary and reversible disease presenting as an unexpected weakening of the left ventricular myocardium. It mainly occurs in individuals who are undergoing sudden and intense stressful conditions. The mortality rate in TCM is between 0% and 8% and the left ventricle function typically regains normality within 1–4 weeks.
During the evaluation of patients who were thought to have suffered a heart attack, it was found that approximately 1%–2% of them were actually affected by TCM. Women in the post-menopausal stage are more prone to this syndrome than men; the reason could be the low levels of estrogen in the body following menopause.
The major complications of TCM are heart failure, left ventricular outflow tract (LVOT) obstruction, and thrombus formation. Some rarer complications are low blood pressure(cardiogenic shock), serious arrhythmias, and pulmonary edema (difficulty in breathing).
Heart Failure
Heart failure is generally a common complication that sets in during the severe stage of TCM in 12-45% of affected individuals. Patients who experience recurrent TCM are more to prone to develop heart failure; however, the probability of recurrence is low.
Individual factors predicting a higher risk of serious heart failure include a reduced left ventricular ejection fraction, older age, elevated troponin levels, and a history of a physical stressor which precipitated TCM. The severity of pulmonary edema caused by LV dysfunction is increased by accompanying LV outflow tract obstruction and mitral regurgitation.
Thrombosis
Thrombosis is a term which indicates the formation of blood clots within the blood vessel, leading to reduced blood flow in the circulatory system. It may occur within the venous or arterial system. The symptoms of thrombosis depend on its position, size, and embolization.
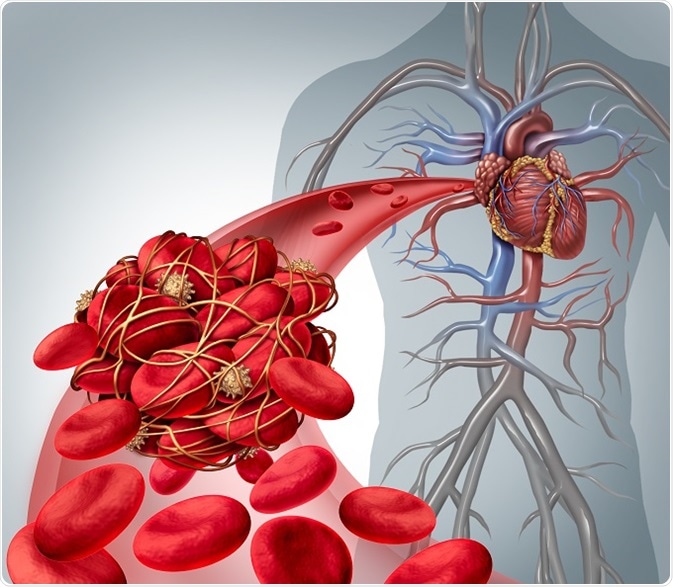
© Lightspring/Shutterstock.com
Blood clots within veins or arteries may result in various disease conditions such as pulmonary embolism (migration and lodging of a clot formed elsewhere into the lungs), myocardial infarction (obstruction of a blood vessel supplying heart muscle), and stroke (obstruction of blood supply to part of the brain).
Marked systolic dysfunction in LV is observed in all patients with TCM. Left ventricular (LV) thrombus apical formation is a known but rare complication of TCM. It occurs because of the stagnation of blood in the akinetic segment. Once the LV function reverts to normal, the use of warfarin to prevent thrombosis is no longer required.
Left Ventricular Outflow Tract Obstruction
Patients with TCM may develop left ventricular outflow tract obstruction (LVOTO). The LVOT refers to the route along which blood first flows along the septal wall to leave the left ventricle through the aortic valve. When the base of the heart shows exaggerated contraction in association with apical hypokinesis, the tract is constricted by this unbalanced contraction of the left ventricle. This leads to an increase in the velocity of blood flow through this pathway during systole (heart chamber contraction).
This accelerated blood flow reduces the blood pressure in the region above the nearby mitral valve. This in turn leads to a sucking forward of the anterior mitral valve leaflet toward the intraventricular septum. This is termed systolic anterior motion of the mitral valve and toward the septum, and it can cause still further blockage of the LVOT, resulting in hypotension.
This complication may be diagnosed by performing catheterization or echocardiography.
Hypotension due to LVOT can be controlled in various ways, such as the use of β-blockers that decrease the excessive contractility of the base of the heart and lower the level of obstruction of the LV outlet. β-blockers also increase the ventricular filling volume during diastole, besides the propranolol-associated reduction in the difference in pressure between the apex of the left ventricle and the LVOT, to reduce the acceleration of blood flow.
A greater blood volume also relieves the obstruction by increasing the functional capacity of the outflow tract, so intravenous fluids may be given to increase the blood volume if pulmonary edema is absent.
The chance of developing life-threatening complications of this syndrome is low, but 20% of patients may suffer from heart failure. Thrombosis and apical rupture may increase the mortality rate in TCM. Patients with a history of psychiatric and pre-existing neurological problems, who suffer complications of TCM, are suggested to seek expert psychiatrist care alongside the cardiac treatment.
Cardiogenic Shock
This phenomenon occurs when the heart muscle fails to pump enough blood into the circulatory system. The main cause of this complication is acute LV dysfunction. Other triggering factors include involvement of the RV, LVOT obstruction, and severe mitral regurgitation, all of which may worsen the severity of TCM. It is a very rare phenomenon but may be lethal if immediate treatment is not provided.
Sources:
- http://ccn.aacnjournals.org/content/29/1/49.full.pdf
- www.mayoclinic.org/.../ovc-20264165
- http://www.cardiomyopathy.org/takotsubo-cardiomyopathy/intro
- https://juniperpublishers.com/jocct/pdf/JOCCT.MS.ID.555597.pdf
- www.nhlbi.nih.gov/.../signs-and-symptoms
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3209596/
- www.bhf.org.uk/.../takotsubo-cardiomyopathy
Further Reading
Last Updated: Aug 23, 2018






















.png)








No hay comentarios:
Publicar un comentario