
FDA Alters Approved Use of Two Checkpoint Inhibitors for Bladder Cancer
July 26, 2018, by NCI Staff
The Food and Drug Administration (FDA) has changed the approved uses of two immunotherapy drugs to treat people with the most common form of bladder cancer, urothelial carcinoma.
Last year, the drugs—pembrolizumab (Keytruda)and atezolizumab (Tecentriq)—received approvalfor the treatment of patients with previously untreated urothelial carcinoma that has spread beyond the bladder. The 2017 approvals covered the use of the drugs for patients who, because of other health-related factors, cannot receive the chemotherapy drug cisplatin, which is a standard treatment for patients with advanced bladder cancer.
Approximately half of people diagnosed with bladder cancer that has spread can’t receive cisplatin, explained Andrea B. Apolo, M.D., of the Genitourinary Malignancies Branch (GMB) in NCI’s Center for Cancer Research.
Last year’s approvals were based on results from two small, early-phase clinical trials. On June 20, however, the agency announced that data from two larger, ongoing clinical trials showed that patients with metastatic bladder cancer treated with either pembrolizumab or atezolizumab died sooner than those treated with a standard chemotherapy regimen.
The worse survival was seen specifically in people whose tumor cells had very low levels of the protein PD-L1.
As a result of the new findings, FDA announced that it was changing the prescribing label for both drugs. Under the change, pembrolizumab and atezolizumab should be used as an initial, or first-line, treatment in only those people with metastatic bladder cancer who can’t receive cisplatin-based chemotherapy and whose tumors have high levels of PD-L1. The assessment of PD-L1 levels must be made using an FDA-cleared test.
Under the labeling change, Dr. Apolo noted, patients who can’t be treated with any platinum-containing therapy can still receive either immunotherapy drug, regardless of their PD-L1 levels.
Following Up on Accelerated Approvals
Pembrolizumab and atezolizumab are both immune checkpoint inhibitors, and both are approved by FDA to treat patients with metastatic bladder cancer that has continued to progress on standard treatments such as combinations of chemotherapy drugs.
The expanded approvals of both drugs as first-line treatments in 2017 were accelerated approvals, based on the findings from smaller clinical trials showing that some patients’ tumors shrank following treatment. Because they were not randomized trials that compared the drugs against standard treatments, however, the trials could not show whether patients who received the immunotherapy drugs lived longer.
Under an accelerated approval, a drug’s manufacturer has to conduct a larger trial to confirm that the drug does indeed have a meaningful benefit for patients, such as improving survival or quality of life.
It was the early analyses of data from two of these confirmatory trials—KEYNOTE-361(pembrolizumab) and IMvigor 130 (atezolizumab)—which showed that patients with low PD-L1 levels who received the checkpoint inhibitor alone “had decreased survival compared to patients who received cisplatin- or carboplatin-based chemotherapy,” the agency reported.
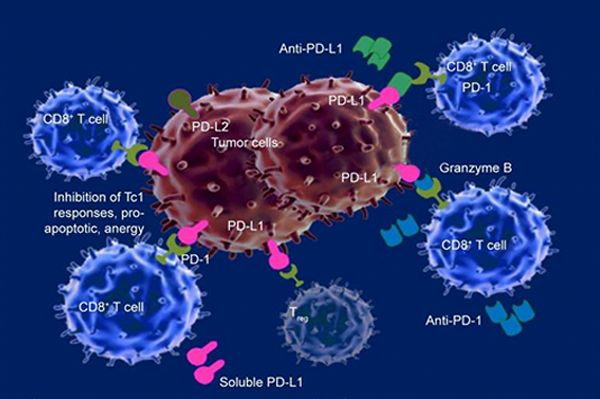
PD-L1 levels have been widely studied as a biomarker for response to treatment with checkpoint inhibitors. PD-L1 on tumor cells is involved in dialing down the immune response, and both pembrolizumab and atezolizumab disrupt that process. Several checkpoint inhibitor approvals have been limited to people whose tumors have elevated PD-L1 levels.
However, using PD-L1 levels to select treatment for these patients “puts oncologist in the difficult position of finding a laboratory that will do the correct assay for that specific therapy,” said Dr. Apolo. “The assays used with atezolizumab and pembrolizumab each look at different cells, the cut-off for a ‘positive’ result is still being fine-tuned for each assay, and some patients may not have tissue available for testing,” she explained.
Also, for patients who are ineligible to receive cisplatin, selecting treatment based on the PD-L1 levels of their tumors “may eliminate a viable, effective treatment option for some patients,” said Dr. Apolo. “Based on the reported studies that led to these approvals, approximately 20%–30% of cisplatin-ineligible bladder cancer patients with low PD-L1 levels had durable responses to atezolizumab or pembrolizumab.”
According to FDA, patients with low PD-L1 levels are no longer being enrolled in the KEYNOTE-361 or IMvigor 130 trials.
Evolving Role of Immunotherapy in Bladder Cancer
It’s not surprising that the patients who received chemotherapy responded well to treatment, said Dr. Apolo, who heads the GMB’s Bladder Cancer Section. “Chemotherapy is very active in patients with urothelial carcinoma,” she explained.
In fact, Dr. Apolo continued, evidence from previous bladder cancer trials has shown that the rates at which patients’ tumors shrink after treatment with first-line chemotherapy regimens that include cisplatin or carboplatin are higher than the rate for cisplatin-ineligible patients treated with a first-line checkpoint inhibitor.
However, patients whose tumors do respond to checkpoint inhibitors tend to maintain those responses for long periods, she said. So the premise in these trials was that these extended responses “would translate into a survival benefit.”
Data on whether survival will be improved for patients with high PD-L1 levels treated with only a checkpoint inhibitor are still not available. In addition, KEYNOTE-361 and IMvigor 130 also have a treatment group that is receiving the immunotherapy drug in combination with chemotherapy, but efficacy data are not yet available for those groups either.
Dr. Apolo stressed that, in patients whose cancer has progressed after chemotherapy treatment, “immunotherapy with checkpoint inhibitors [alone] is still the standard of care.”





















.png)










No hay comentarios:
Publicar un comentario