
Managing Cancer Pain: Are Better Approaches on the Horizon?
January 23, 2019, by NCI Staff
Pain is a common and much-feared symptom among people being treated for cancer and long-term survivors. Cancer pain can be caused by the disease itself, its treatments, or a combination of the two. It may be short-lived or chronic, and for some people it can persist long after treatment ends.
And more and more people are living with cancer-related pain. Thanks to improved treatments, people are living longer with advanced cancer and the number of long-term cancer survivors continues to grow. In addition, because cancer occurs at a higher rate in older individuals, the worldwide prevalence of cancer is increasing as people around the globe are living longer.
The increased prevalence of cancer pain and the impact of the opioid epidemic on cancer pain management—and on managing chronic pain in general—have sparked renewed interest in developing new, nonaddictive pain medications as well as nondrug approaches for managing chronic pain.
Understanding cancer pain is a challenging problem, and the universe of researchers working in this area is small, said Ann O’Mara, Ph.D., R.N., M.P.H., who recently retired as head of palliative research in NCI’s Division of Cancer Prevention. Nevertheless, scientists who study cancer pain are cautiously optimistic that better treatments are on the horizon.
Thanks in part to the development of animal models of some types of cancer pain, researchers are beginning to better understand its underlying biology. In particular, scientists are identifying molecules that generate pain signals and gaining insights into how the nervous system transmits these signals from the pain site to the brain, where pain is perceived.
This research has led to numerous ongoing clinical trials, including some large studies that are typically required to gain Food and Drug Administration approval, of experimental therapies to prevent pain.
Insights on Cancer-Induced Bone Pain Leading to New Treatments
One of the most common types of cancer pain is bone pain. Cancer-induced bone pain occurs when metastatic tumors of cancers that start in other parts of the body grow in the bone marrow, the sponge-like tissue in the center of most bones. In fact, bone pain may be the first symptom of several forms of cancer, including prostate and lung cancer, said Patrick Mantyh, Ph.D., J.D., of the University of Arizona in Tucson.
Cancer-induced bone pain also occurs in people with primary bone cancers (tumors that begin in bone tissue), such as osteosarcoma, which are far less common than cancers that spread to the bones.
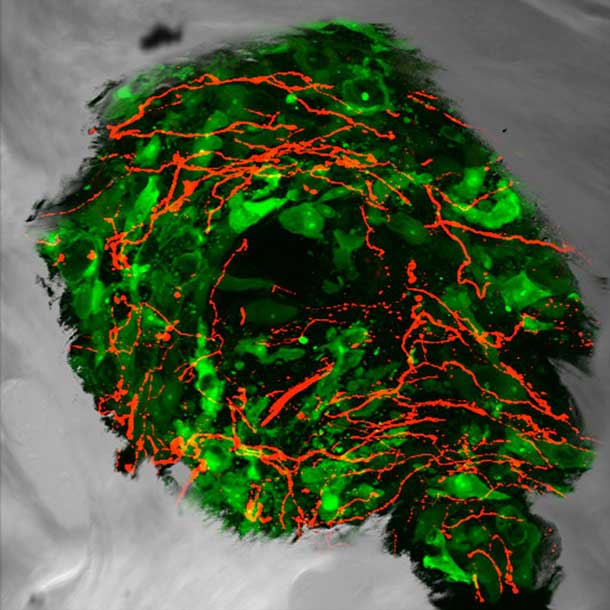
In 1999, Dr. Mantyh’s lab developed the first animal model that appears to mirror what occurs in humans with pain from cancer that has spread, or metastasized, to the bone. Using that mouse model, Dr. Mantyh’s team found that tumors in bone stimulate the sprouting of pain-transmitting nerve fibers near the tumor.
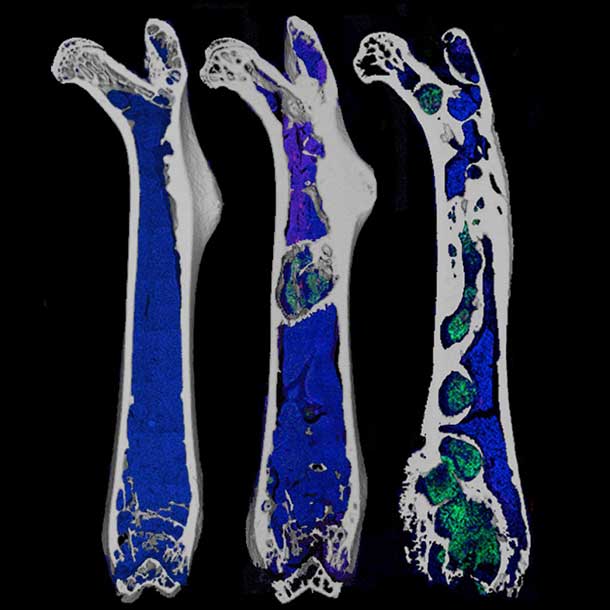
Once tumor cells are established in the bone marrow, Dr. Mantyh said, they hijack the molecules that regulate cells involved in breaking down bone, called osteoclasts. As a result, “the osteoclasts get bigger and then they avidly digest bone,” he explained.
To digest bone, osteoclasts create an acidic environment that “is almost like pouring battery acid on bone,” Dr. Mantyh continued. The causes of bone cancer pain are twofold, he said. First, sensory neurons, or nerve fibers, in bone “detect the acidic environment and signal it as pain.” Second, excess osteoclast activity results in microfractures or full fractures of bone that can cause extreme pain.
Studies using the lab’s mouse model led to human trials of denosumab (Prolia), the first drug approved to treat bone pain caused by metastatic cancer, and of bisphosphonates like alendronate (Fosamax), another first-line therapy for cancer-induced bone pain. Both denosumab and bisphosphonates, which were originally developed to treat osteoporosis, help maintain bone integrity by reining in osteoclast activity.
A potential new treatment for bone pain due to metastatic cancer is an antibody called tanezumab, which blocks the activity of a pain-signaling molecule called nerve growth factor (NGF). Dr. Mantyh’s team showed, in mice, that tanezumab blocks nerve sprouting in bone and reduces the development of late-stage cancer pain.
Tanezumab is now being tested in phase 3 clinical trials for cancer-induced bone pain. A related approach seeks to block the actions of NGF by blocking its receptor, known as TrkA (tropomyosin receptor kinase A), on sensory nerve fibers, Dr. Mantyh said.
There’s also a keen interest in using cannabinoids—chemicals found in marijuana—to treat cancer-induced bone pain and some other types of cancer pain, Dr. O’Mara said, although, so far, research in this area is limited to studies in animal models.
For example, work by Todd Vanderah, Ph.D., of the University of Arizona, has shown that cannabinoids can reduce severe bone pain and also suppress cancer growth and reduce bone loss in a mouse model of breast cancer that has spread to the bone.
Looking into the Causes of Oral Cancer Pain
The most common cancer types, such as breast, lung, prostate, and colon cancer, rarely cause pain at the site where they originate. However, pain in the head and neck from oral cancer is notable for its intensity and prevalence, with approximately 70%–75% of patients with oral cancer experiencing pain, said Brian Schmidt, D.D.S., M.D., Ph.D., of New York University's College of Dentistry.
Dr. Schmidt noted that oral cancer pain is persistent because the tongue and floor of the mouth (the areas most commonly affected by oral cancer) are disturbed when a patient talks, chews, or swallows. Pain occurs when substances produced and secreted by a tumor activate nearby pain-sensing neurons, which then transmit pain signals to the central nervous system—and the stimulation from simply talking or swallowing exacerbates this effect.
To study oral cancer pain, Dr. Schmidt collects tumor-produced, pain-causing substances during surgery with a technique called microdialysis. “The cancer tissue degenerates rapidly after surgery. By sampling the cancer microenvironment with the tumor in place, we glean a more accurate understanding of how the tumor causes pain,” Dr. Schmidt said.
In other cases, Dr. Schmidt removes small pieces of tumor as well as normal tissue from an adjacent area in the mouth. From these samples, his lab team works to identify pain-promoting substances found in the cancerous tissue but not the normal tissue.
Among their prime suspects for causing oral cancer pain are proteases—enzymes that break down proteins and can help cancers spread by destroying surrounding tissues. Proteases can also latch onto, and activate, a receptor molecule on neurons called protease-activated receptor 2, or PAR2. When proteases activate PAR2 on neurons, PAR2 can cause other pain receptors on neurons to become more sensitive,” Dr. Schmidt said. As a result, he continued, “a stimulus that is not normally painful, such as a potato chip hitting the tongue, can become exquisitely painful.”
Dr. Schmidt and a collaborator, Nigel Bunnett, Ph.D., of Columbia University, are studying a new class of drugs that block PAR2 to treat oral cancer pain. In addition, Dr. Schmidt’s team is investigating several other substances that may contribute to oral cancer pain. These include NGF, a culprit in cancer-related bone pain, and endothelin-1, a pain-producing molecule notable for its presence in snake venom.
Pain as a Side Effect of Treatment

Pain can also arise due to chemotherapy-induced peripheral neuropathy (CIPN), a serious side effect of many chemotherapy drugs. Peripheral neuropathy results from damage to nerves in the extremities, like fingers and toes, and causes pain, numbness, and tingling. (Cancer treatments such as surgery and radiation, as well as the disease itself, may also cause peripheral neuropathy in patients and survivors.)
CIPN is the most common reason that patients must reduce their dose of chemotherapy. Some may even stop cancer treatment entirely because the effects of CIPN are so debilitating and distressing. And it’s not just the painful aspect of neuropathy that’s problematic.
“The nonpainful components [such as numbness in the hands and feet] also greatly impact patient function and well-being,” said Patrick Dougherty, Ph.D., of the department of pain medicine at the University of Texas MD Anderson Cancer Center.
A recent study led by Igor Spigelman, Ph.D., of the UCLA School of Dentistry, showed that a synthetic cannabinoid suppressed CIPN symptoms in both male and female rats. This cannabinoid is one of a series of synthetic cannabinoids that Dr. Spigelman and Herbert Seltzman, Ph.D., of the Research Triangle Institute in North Carolina, have developed that appear not to affect the central nervous system and that thus avoid the cognitive effects caused by other cannabinoids, such as euphoria, addiction, and impaired function.
Only one drug, duloxetine (Cymbalta), has been shown to reduce pain due to CIPN in people in a phase 3 clinical trial, and that effect is very modest, Dr. Dougherty said.
Scientists don’t yet fully understand the mechanisms that underlie CIPN, but a combination of animal and human studies is yielding new insights, Dr. Dougherty added. The general idea, he explained, is that the chemotherapy drugs that cause CIPN do so by stressing neurons, leading to nerve inflammation and damage.
Researchers are investigating agents that could target the source of the problem and reverse or, ideally, prevent CIPN rather than just relieve symptoms. Some of these agents also have known antitumor effects, making them especially attractive, because a key concern in developing drugs to prevent CIPN is that they could interfere with treatment of the cancer.
“Some new types of agents are coming to clinical trials, and right now the data [from animal studies] is very promising,” Dr. Dougherty said.
Drugs that block the actions of histone deacetylase (HDAC), which are already being tested in clinical trials for their potential to enhance the effects of chemotherapy, are just one of many possible targeted therapies being studied for CIPN. Studies in animal models have shown that certain HDAC inhibitors can prevent and reverse CIPN.
However, when it comes to new drugs to treat or prevent CIPN, Dr. Dougherty said, “we are still very much in a discovery mode.”
A Role for Non-Drug Approaches
Researchers are also investigating non-drug approaches for relieving CIPN and other chronic cancer-related pain, explained Diane St. Germain, RN, MS, who manages a grant portfolio focused on palliative research in NCI's Division of Cancer Prevention.
For example, there is great interest in the use of acupuncture, as well as behavioral approaches such as yoga, Tai Chi, and mindfulness meditation, for pain relief, said Linda Porter, Ph.D., director of the Office of Pain Policy at the National Institute of Neurological Disorders and Stroke, and many of these approaches are being tested in clinical trials.
NIH Initiative to Spur Research on Non-Addictive Pain Treatments
One initiative expected to speed research on new, safer treatment options for pain management in general is the NIH Helping to End Addiction Long-term (HEAL) Initiative. Enhancing pain management is one of two major components of HEAL, which NIH launched to provide scientific solutions to the opioid crisis. This component of HEAL will fund research to meet the following goals:
- Understand the biological underpinnings of chronic pain
- Accelerate the discovery and preclinical development of non-addictive pain treatments
- Advance new non-addictive pain treatments through the clinical pipeline
- Establish the best pain management strategies for acute and chronic pain conditions
Behavioral interventions for cancer pain are generally used as an adjunct to medication, said Tamara Somers, Ph.D., a clinical psychologist and behavioral scientist at Duke University School of Medicine.
Dr. Somers studies behavioral pain management approaches such as cognitive behavioral therapy(CBT), which is designed to teach patients pain management skills to improve their pain coping strategies and decrease stress that can lead to more pain.
Clinical trials have shown that behavioral interventions “can decrease pain and disability for patients with cancer,” Dr. Somers said. “But CBT for pain management can also provide people with coping skills to use in the face of pain, so even if their pain persists at some level, they can continue doing what they need to do, or want to do, day to day.
“We know that these coping skills help people manage their pain,” Dr. Somers continued. But behavioral pain management usually requires in-person therapy sessions at a medical center and a significant time commitment, and “at many places there isn’t even a therapist available who’s been trained to do these interventions,” she said.
To address those challenges, Dr. Somers is studying whether a shorter or lesser “dose” of a behavioral pain intervention can still provide benefits. In an ongoing NCI-sponsored clinical trial, she is examining the response of breast cancer patients with moderate or severe pain to differing doses of pain coping skills training. The aim is to figure out “who needs what dose of a behavioral cancer pain intervention to benefit, with the end goal of making this approach more accessible for patients,” Dr. Somers said.
Dr. Somers is also looking at alternatives to in-person therapy for people with chronic cancer pain, including mobile health interventions. Such interventions can include videoconferences and electronic tablet kiosks in community medical centers for patients who can’t access technology at home, such as medically underserved populations in rural areas.
One challenge in using behavioral interventions to manage cancer pain, Dr. O’Mara said, “is that, unlike taking a pill, it requires a commitment of time and effort from the patient.” One question, then, is, “how to empower patients to be committed to these approaches,” which may not eliminate pain but will help them live with it, she said.
Other Challenges of Studying and Managing Pain
When it comes to controlling pain, it’s preferable to start treatment early in the course of the disease—and, ideally, before pain develops in the first place, Dr. Mantyh said. But that can be challenging, he said, because oncologists tend to be more focused on “treating the tumor … and it can be hard to get buy-in from them to give [a treatment] early in the disease to control pain.”
One concern among oncologists, Dr. Dougherty said, is that drugs to prevent pain might interact and interfere with anticancer treatments. “You want patients to survive the therapy first, and an agent that might interact with a cancer therapy would have a clear downside,” he said.
However, he added, it’s important to address nerve-related pain such as CIPN as soon as possible, because once pain becomes chronic, “a patient’s nervous system starts to change and try to adapt to that condition … [so] now you have a new problem of trying to get the nervous system to go back to where it was.”
Another complicating factor is that men and women may have different biological responses to pain, Dr. Dougherty said. His lab is comparing human sensory neurons from painful and nonpainful areas in patients with CIPN to examine its biological basis. As-yet-unpublished findings indicate that, “as has been suggested in animal studies, there are [genetic] differences between men and women” in the way that neurons respond to chemotherapy-induced stress, suggesting that therapies for CIPN will have to be specifically tailored based on a patient’s sex, he said.
One thing is clear, scientists working in this area agree: Improving the understanding of pain and using that knowledge to guide the discovery and development of new treatments is critical for patients’ physical and mental well-being.
“Most people would agree that if you can control the pain, that will probably make a difference in extending a patient’s lifespan just because they are able to exercise, maintain a social life, and try to maintain a healthy lifestyle,” Dr. Mantyh said. “If you can maintain a cancer patient’s functional status, you dramatically improve their quality of life. And that, along with being able to stay on their cancer therapies … is what it’s all about.”























.png)








No hay comentarios:
Publicar un comentario